
The surgical management of patients with tetralogy of Fallot and significant right ventricular outflow tract obstruction (RVOTO) remains controversial. The authors describe the use of a monocusp in patients with right ventricular outflow tract obstruction.
Patient Selection
The surgical management of patients with tetralogy of Fallot and significant right ventricular outflow tract obstruction (RVOTO) remains controversial. For patients who have a congenitally small pulmonary valve annulus who are not candidates for a valve-sparing repair, there have historically been two options: (1) transannular patch or (2) valved conduit insertion. The advantage of the transannular patch is that it relieves the RV pressure immediately and the child usually will not require reoperation for RV outflow tract stenosis. A disadvantage of this technique is the sudden hemodynamic change for the RV from a pressure-loaded to a volume-loaded ventricle, which, when combined with VSD closure on one side and ventriculotomy on the other, often causes temporary RV dysfunction. The chronic volume overload can lead to ventricular dysfunction from chronic pulmonary valve insufficiency, and require late pulmonary valve insertion [1]. The advantage of the valved conduit technique is that it results in a reliable, fully competent pulmonary valve. This is particularly useful in patients who have peripheral unrepaired pulmonary stenosis. The disadvantage is that all conduits (or pulmonary valves) are subject to progressive stenosis, either from patient growth or calcification of the valves, and conduit replacement is eventually needed. An interesting alternative strategy is the creation of a monocusp RV outflow tract patch. A monocusp may be created with autologous or bovine pericardium [2], homograft pulmonary valve cusp, or as reported in this technique section, the use of PTFE pericardial membrane (0.1 mm PTFE patch) [3]. The monocusp has been shown, particularly in the immediate postoperative period, to prevent pulmonary valve insufficiency [4]. This may be associated with faster recovery of RV function, a lower central venous pressure, and less chest tube drainage. The construction of the monocusp is simple, very inexpensive, and reproducible. The potential disadvantage in comparison to insertion of a pulmonary valve or valved conduit is that, at least in some patients, there appears to be a faster progression to recurrent pulmonary valve insufficiency, although late stenosis is rarely, if ever, seen using this technique.
The patient selected for this procedure would be one for whom the surgeon would consider either a transannular patch or a pulmonary valve insertion at the time of initial tetralogy of Fallot repair, or a patient having a reoperation after initial transannular patch or valved conduit placement.
Operative Steps
Pulmonary Artery Incision
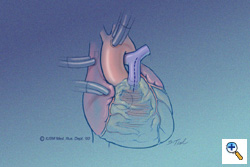 The patient has been placed on cardiopulmonary bypass with aortic and bicaval venous cannulation. The dotted line indicates the vertical incision to be made in the main pulmonary artery. Through this incision the pulmonary valve and annulus can be inspected. If possible, a pulmonary valvotomy can be performed and the annulus measured with dilators. In patients with moderate to severe hypoplasia of the annulus (generally more than 1 mm smaller than a -1 Z value), a transannular repair can be performed with the use of the monocusp. The other indication for the use of the monocusp would be a post-repair RVOT gradient greater than 25-30 mmHg following a valve-sparing attempt. This portion of the operation can be performed after the ventricular septal defect (dotted line circle) has been closed and the aortic cross clamp removed.
The patient has been placed on cardiopulmonary bypass with aortic and bicaval venous cannulation. The dotted line indicates the vertical incision to be made in the main pulmonary artery. Through this incision the pulmonary valve and annulus can be inspected. If possible, a pulmonary valvotomy can be performed and the annulus measured with dilators. In patients with moderate to severe hypoplasia of the annulus (generally more than 1 mm smaller than a -1 Z value), a transannular repair can be performed with the use of the monocusp. The other indication for the use of the monocusp would be a post-repair RVOT gradient greater than 25-30 mmHg following a valve-sparing attempt. This portion of the operation can be performed after the ventricular septal defect (dotted line circle) has been closed and the aortic cross clamp removed.
Ventriculotomy
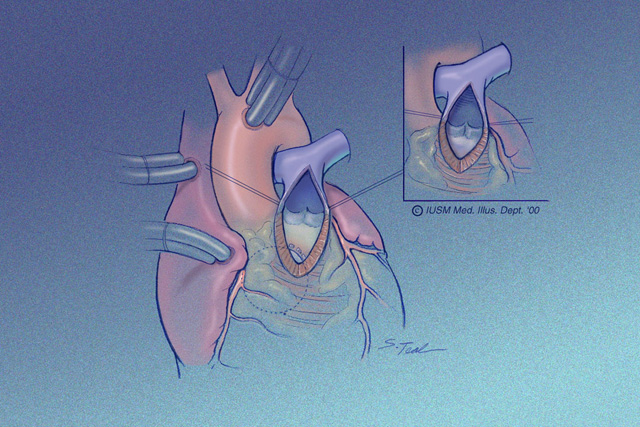 The ventriculotomy is carried onto the RV only as far as necessary to alleviate the infundibular narrowing. This incision in general is 1-2 cm in length, but may be longer in patients with a long, narrowed infundibular septum. The ventriculotomy is also longer if transventricular rather than transatrial VSD closure is to be performed. At the mid-point of the incision, usually the site of the pulmonary valve annulus, the edges of the ventriculotomy are retracted with stay sutures. The functional remnant of pulmonary valve leaflets posteriorly are left intact.
The ventriculotomy is carried onto the RV only as far as necessary to alleviate the infundibular narrowing. This incision in general is 1-2 cm in length, but may be longer in patients with a long, narrowed infundibular septum. The ventriculotomy is also longer if transventricular rather than transatrial VSD closure is to be performed. At the mid-point of the incision, usually the site of the pulmonary valve annulus, the edges of the ventriculotomy are retracted with stay sutures. The functional remnant of pulmonary valve leaflets posteriorly are left intact.
PTFE Monocusp Creation
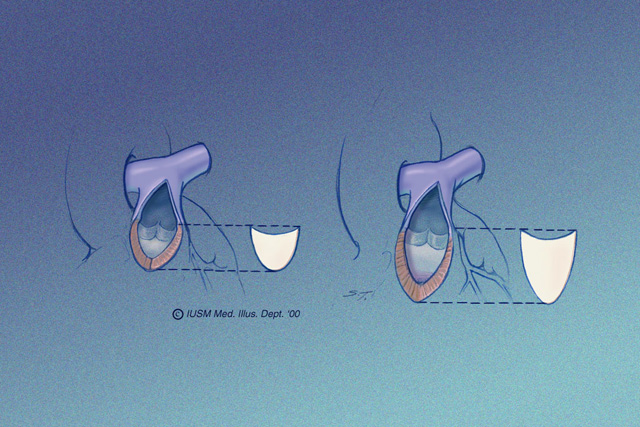 A bullet-shaped piece of 0.1-mm PTFE (Preclude® pericardial membrane, W.L. Gore & Associates, Flagstaff, AZ) is fashioned as shown. The membrane is placed in the ventricular portion of the opening, allowing it to lay flush along the ventricular walls and conal septum, thereby maximizing surface area coaptation. The edges of the PTFE are traced with a marking pen according to their point of contact with the epicardial surface and the material is cut to the dimensions as outlined. This complements the RVOT anatomic geometry. The illustration on the left shows a short RVOT incision, the illustration on the right shows an extended RVOT incision. The monocusp must be longer, obviously, for a patient with a longer ventriculotomy. This is a key technical point. The monocusp is not constructed to approximate the size of the remaining pulmonary valve leaflets, it is constructed to approximate the size of the ventriculotomy opening. The leading edge of the proposed monocusp is actually flat. It appears curved in these illustrations to show the depth of the leading edge when it fills the RVOT.
A bullet-shaped piece of 0.1-mm PTFE (Preclude® pericardial membrane, W.L. Gore & Associates, Flagstaff, AZ) is fashioned as shown. The membrane is placed in the ventricular portion of the opening, allowing it to lay flush along the ventricular walls and conal septum, thereby maximizing surface area coaptation. The edges of the PTFE are traced with a marking pen according to their point of contact with the epicardial surface and the material is cut to the dimensions as outlined. This complements the RVOT anatomic geometry. The illustration on the left shows a short RVOT incision, the illustration on the right shows an extended RVOT incision. The monocusp must be longer, obviously, for a patient with a longer ventriculotomy. This is a key technical point. The monocusp is not constructed to approximate the size of the remaining pulmonary valve leaflets, it is constructed to approximate the size of the ventriculotomy opening. The leading edge of the proposed monocusp is actually flat. It appears curved in these illustrations to show the depth of the leading edge when it fills the RVOT.
Monocusp Insertion
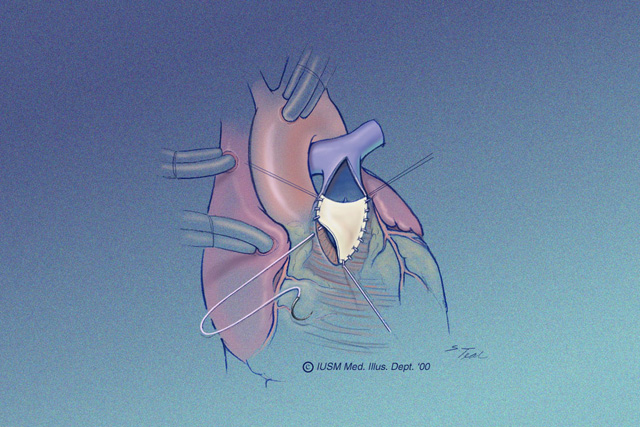 The monocusp is sutured to the ventriculotomy opening with running 6-0 PTFE suture. The suturing begins at the proposed hinge point and extends onto the epicardial surface of the ventricle with bites that include at least one-half the depth of the myocardium. Care is taken to ensure that the superior edge of the monocusp matches that of the retained posterior leaflets.
The monocusp is sutured to the ventriculotomy opening with running 6-0 PTFE suture. The suturing begins at the proposed hinge point and extends onto the epicardial surface of the ventricle with bites that include at least one-half the depth of the myocardium. Care is taken to ensure that the superior edge of the monocusp matches that of the retained posterior leaflets.
PTFE Outflow Tract Patch
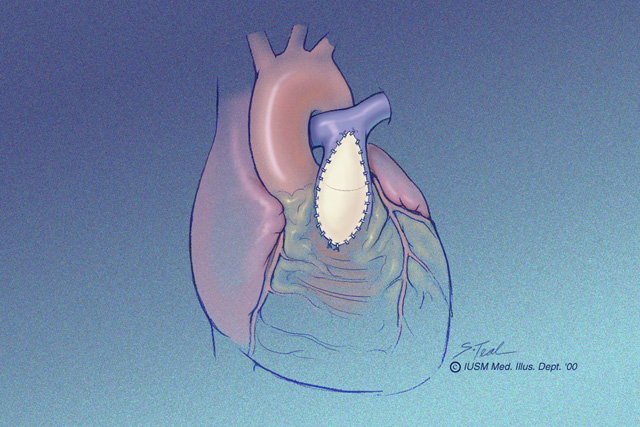 The PTFE outflow tract patch forms a roof over the monocusp. This patch is sutured to the main pulmonary artery and to the ventriculotomy edge and in effect reinforces the suture line of the monocusp itself to the ventriculotomy opening. The dotted line in the mid-portion of this illustration shows the location of the monocusp within the PTFE outflow tract patch. This patch is also sutured in place using running 6-0 PTFE suture. The patch is constructed with 0.4-mm thickness PTFE cardiovascular patch in an elongated teardrop configuration.
The PTFE outflow tract patch forms a roof over the monocusp. This patch is sutured to the main pulmonary artery and to the ventriculotomy edge and in effect reinforces the suture line of the monocusp itself to the ventriculotomy opening. The dotted line in the mid-portion of this illustration shows the location of the monocusp within the PTFE outflow tract patch. This patch is also sutured in place using running 6-0 PTFE suture. The patch is constructed with 0.4-mm thickness PTFE cardiovascular patch in an elongated teardrop configuration.
Monocusp Function
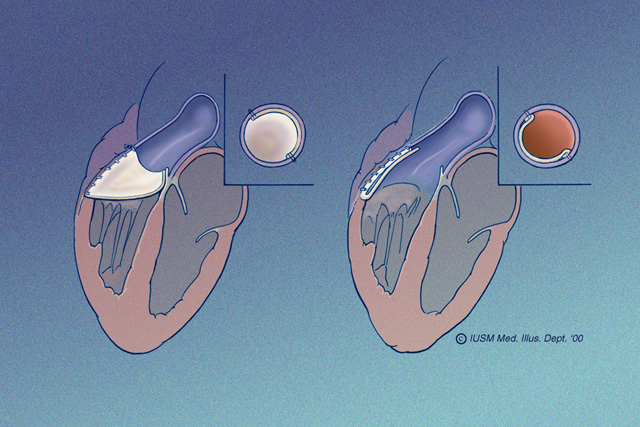 The functional characteristics of the monocusp are demonstrated here. The illustration on the left shows the monocusp in diastole. Blood from the pulmonary artery has filled the monocusp and presses it against the septum and remaining posterior pulmonary valve leaflet. This is the coaptation site of the monocusp. In the illustration to the right, the monocusp is in the open position; this would be during systole. The monocusp is flush with the RVOT anterior RV wall and PTFE outflow tract patch. The function of the monocusp can be evaluated intraoperatively with transesophageal echocardiography.
The functional characteristics of the monocusp are demonstrated here. The illustration on the left shows the monocusp in diastole. Blood from the pulmonary artery has filled the monocusp and presses it against the septum and remaining posterior pulmonary valve leaflet. This is the coaptation site of the monocusp. In the illustration to the right, the monocusp is in the open position; this would be during systole. The monocusp is flush with the RVOT anterior RV wall and PTFE outflow tract patch. The function of the monocusp can be evaluated intraoperatively with transesophageal echocardiography.
Prior RVOT Conduit
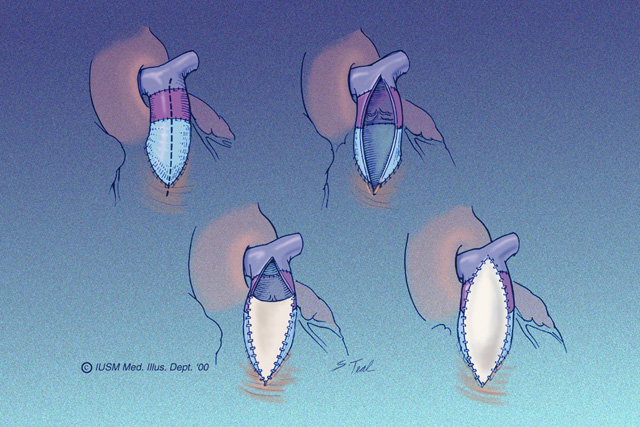 For the patient who has had a previous RVOT conduit that has become stenotic, the PTFE monocusp may be used as an alternative to valve or conduit replacement. This illustration shows a vertical incision through the extent of the previously placed valved conduit. The previously placed valve is partially excised. A hinge point is selected for the monocusp, usually at the mid-portion of the old conduit. The monocusp valve is constructed as shown in the lower left panel. Finally, a 0.4-mm thickness PTFE cardiovascular patch is used, again in a teardrop configuration, to create a roof over the monocusp patch. Sizing of the monocusp is essentially the same as with other repairs; the material must have adequate length and width in order to have sufficient surface area contact against the posterior wall.
For the patient who has had a previous RVOT conduit that has become stenotic, the PTFE monocusp may be used as an alternative to valve or conduit replacement. This illustration shows a vertical incision through the extent of the previously placed valved conduit. The previously placed valve is partially excised. A hinge point is selected for the monocusp, usually at the mid-portion of the old conduit. The monocusp valve is constructed as shown in the lower left panel. Finally, a 0.4-mm thickness PTFE cardiovascular patch is used, again in a teardrop configuration, to create a roof over the monocusp patch. Sizing of the monocusp is essentially the same as with other repairs; the material must have adequate length and width in order to have sufficient surface area contact against the posterior wall.
Preference Card
Patch/Membrane
- 0.4 mm thickness cardiovascular patch (GORE-TEX® Cardiovascular Patch, W.L. Gore & Associates, Flagstaff, AZ)
- 0.1 mm thickness pericardial membrane (PRECLUDE® Pericardial Membrane, W.L. Gore & Associates, Flagstaff, AZ)
Sutures
- 6-0 PTFE suture (GORE-TEX® Suture, W.L. Gore & Associates, Flagstaff, AZ)
Equipment/Instruments
- Intraoperative transesophageal echocardiography
- Hegar or Amato dilators
Tips & Pitfalls
This operation lends itself well to following the carpenter’s rule: measure twice, cut once. If the PTFE monocusp patch is too small or too large, it may not work properly and would require reinstitution of cardiopulmonary bypass and revision of the patch. However, multiple suture lines in the RVOT will result in injury to the muscle in this area and make it difficult to obtain hemostasis. This also might place the patient at risk for development of a pseudoaneurysm through the suture line if there is sufficient damage to the edge of the muscle in this area. This technique is probably not suitable for patients who rely upon a competent pulmonary valve, i.e., patients with tetralogy of Fallot and absent pulmonary valve, or patients with significant peripheral pulmonary stenosis either congenital or secondary to previous aorto-pulmonary shunts. Patients with significant pulmonary hypertension might also be better served with the use of a valved conduit.
Results
At Indiana University, between June 1990 and June 1999, 158 patients underwent either PTFE monocusp RVOT reconstruction (n=115 patients, 120 implants) or non-valved transannular repair (n=43) [5]. Follow-up data are available at a mean of 2.6 years. There was no difference in postoperative mortality (2.6% versus 2.3%). There were no late deaths. Perioperative complications were not significantly different, nor were total hospital days. However, a significant difference in intensive care unit utilization (3.6 versus 5.8 days) favored monocusp patients. Patients with, specifically, tetralogy of Fallot or pulmonary atresia with ventricular septal defect undergoing monocusp implant demonstrated a trend towards improved survival when compared with transannular repairs. Intraoperative pulmonary insufficiency was graded mild in the monocusp group and moderate-to-severe in the transannular group. Progressive monocusp regurgitation occurred (mild to moderate) but remained significantly less than the transannular patch repairs.
Use of a PTFE monocusp valve prevents short-term and significantly reduces mid-term pulmonary valve insufficiency. It is inexpensive, easy to construct, and demonstrates no evidence of stenosis, calcification, or embolization. Despite slightly longer cardiopulmonary bypass times, it reduces intensive care unit stay and, in both tetralogy of Fallot and pulmonary atresia/VSD patients, its use decreases operative morbidity and mortality.
References
- Discigil B, Dearani JA, Puga FJ, et al. Late pulmonary valve replacement after repair of tetralogy of Fallot. J Thorac Cardiovasc Surg 2001;121:344-51.
- Gundry, SR. Pericardial and synthetic monocusp valves: indication and results. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 1999;2:77-82.
- Turrentine MW, McCarthy RP, Vijay P, et al. Polytetrafluoroethylene monocusp valve technique for right ventricular outflow tract reconstruction. Ann Thorac Surg 2002;74:2202-5.
- Gundry SR, Razzouk AJ, Boskind JF, et al: Fate of the pericardial monocusp pulmonary valve for right ventricular outflow tract reconstruction: Early function, late failure without obstruction. J Thorac Cardiovasc Surg 1994;107:908-13.
- Turrentine MW, McCarthy RP, Vijay P, et al. PTFE monocusp valve reconstruction of the right ventricular outflow tract. Ann Thorac Surg 2002;73:871-80.
